
Prevalence of neck/shoulder pain among public hospital workers in China and its associated factors: a cross-sectional study

Participants
From September to November in 2019, a cross-sectional survey was implemented in Shandong province, China. Based on hospital functions, facilities, technical level and hospital scale, the public hospitals in China were classified into three levels by Health Administration of China, namely, primary hospitals, secondary hospitals and tertiary hospitals24. The primary hospital is a grass-roots hospital, or community hospital that directly provides comprehensive services of medical treatment, prevention, rehabilitation and health care for the community, and it is a primary health care institution. The secondary hospital is a regional hospital that provides medical and health services across several communities, and the tertiary hospital is a cross regional, provincial, municipal and nationwide hospital providing medical and health services. First, 26 primary hospitals, 8 secondary hospitals and 3 tertiary hospitals were randomly selected from among its according level hospitals, respectively. Then of the above 37 hospitals selected, the workers in active service and without exclusion criteria were all invited to participate in the survey. Exclusion criteria were: part-time workers, or workers with traffic accident or trauma related to the neck/shoulder region, tumor, congenital diseases related to neck and/or shoulder region such as spinal stenosis, and systemic diseases such as rheumatoid arthritis, diabetes and psychiatric disease. Exclusion criteria were outlined in the informed consent and the workers themselves decided whether to participate in the survey voluntarily. The paper-based questionnaire used in the study was disseminated to every worker at their weekly meeting and collected next day or next meeting. The hospital workers were divided into four groups according to the trial regulations on positions of health care professionals released by China central leading group for the reform of professional titles25: clinicians including physicians and surgeons, nurses, other healthcare technicians, and managers and supporting staff. Other healthcare technicians included pharmacist, laboratory personnel, pathologist, sonographer, radiologist, etc. Managers and supporting staff consisted of administrative personal, financial staff, logisticians, etc. In total, 30,520 public hospital workers including 11,593 clinicians, 13,269 nurses, 3443 other healthcare technicians, and 2215 managers and supporting staff, completed our questionnaire and 4839 failed to participate. Of the 30,520 hospital workers, 14,211 workers were from primary-level hospitals, 9998 from secondary hospitals and 6311 from tertiary hospitals. After checking, 973 questionnaires were excluded due to incompletely filling and 29,547 valid questionnaires were analyzed for the study. Thus the response rate of the study was 83.6%.
The study was approved by the Ethics Committee of Shouguang People’s Hospital, Health Commission of Weifang City (wfwsjk_2019_201) and Health Commission of Shandong Province (2016WS0593). All methods in the study were carried out in accordance with the relevant guidelines and regulations of the Declaration of Helsinki and written informed consent was obtained before the hospital workers took part in the survey.
Questionnaire
A self-administered paper-based questionnaire was developed for the study and was revised after pilot study.
The final questionnaire consisted of three parts. Part one was general information including sex, age, height (cm), weight (kg), educational level (lower than junior college, junior college, bachelor, master or above), smoking (never smoked, ex-smoker, current smoker), and physical exercise in leisure time (never/almost never, sometimes, often).
Part two was NSP information. The information on NSP was assessed by the Nordic Musculoskeletal Questionnaire (NMQ)26, which has been systematically translated into the Chinese language and been validated in the Chinese population27,28,29,30. The participants were asked whether they had experienced pain or discomfort in the neck and/or shoulder region lasting for at least 24 h, 7 days, and 3 months during the previous 12 months. If a participant suffered from pain or discomfort lasting for at least 3 months in the past 12 months in the neck and/or shoulder region, then chronic NSP was considered. Participants suffering from NSP lasting for at least 24 h needed to answer questions on sick leave absence due to NSP (yes or no).
Section three dealt with work characteristics, occupational ergonomic and computer-related factors, mainly derived from the ISO recommendations and the standardized Dutch Musculoskeletal Questionnaire (DMQ)31, of which the Chinese version has been validated and widely used in different occupations of Chinese population30,32. In this study, the questions which might be associated with NSP were chosen, including questions on force, dynamic and static load, repetitive load, other ergonomic factors, standing, walking, sitting and working in uncomfortable postures. Occupational ergonomic factors were measured using a dichotomous scale (no/yes) and the Chinese version of the DMQ has been detailed in our previous studies3,4. Work characteristics included hospital level, work position, and work hours per week (< 40 h, 40–45 h, > 45 h). Computer using information was measured by hospital workers themselves. Distance of the keyboard to the edge of a desk was defined by distance between the g-h point of the keyboard and the edge of the desk.
Statistical analysis
SPSS 25.0 was applied for statistical analysis. Differences between different hospital-level workers and between different groups of hospital workers were analyzed by one-way analysis of variance, chi-square test, or rank sum test. As the odds ratios calculated by logistic regression analysis might overestimate the relative risks when the prevalence was not uncommon, such as over 10%33,34,35, thus log-binomial regression analysis based on generalized linear model was adopted to analyze the association of potential influencing factors including workload, individual, ergonomic and computer-related factors with chronic NSP. Adjusted prevalence ratios (PR) and 95% confidence intervals (95% CI) were calculated in the log-binomial regression analysis with chronic NSP as outcome variable. In order to better identify the confounding variables and estimate the effects of exposure variables, the directed acyclic graph36,37,38 was used. Adjustment for the minimum sufficient set of confounders in the log-binomial analyses was determined by the hypothesized directions of relationship between study variables, depicted in Fig. 1. In model 1 adjusted by age (< 30, 30–40, 40–50, > 50 years old) and sex, hospital level, employment position and other individual factors were considered as the exposure variables and in model 2 adjusted by hospital level, employment position, age and sex, the exposure variables were employment status and other individual factors. In model 3 adjusted by hospital level, employment position, employment status, age and sex, workload, ergonomic factors and other individual factors were the exposure variables and in model 4 adjusted by workload, hospital level, employment position, employment status, age and sex, the exposure variables were computer-related factors and other individual factors. In this study the statistical significance for all tests was set at 0.05.
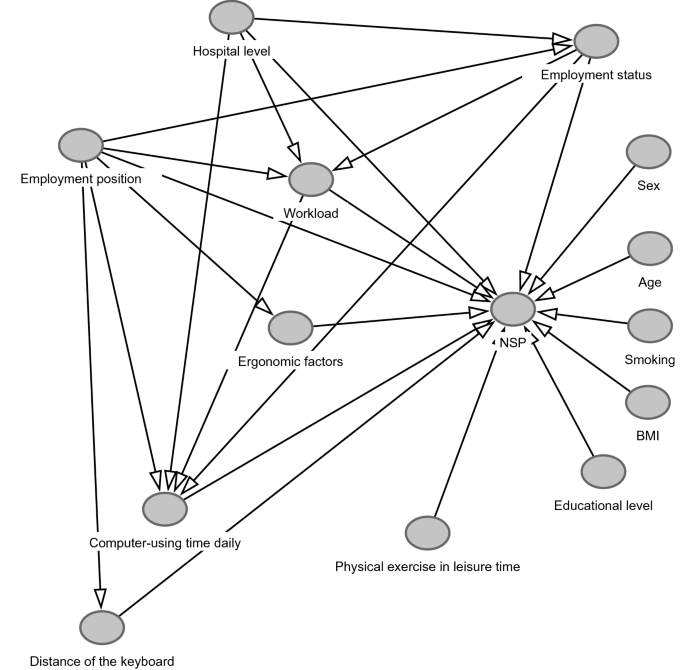
The hypothesized directions of relationship between study variables.
link





